
‘Distal Tibiofibular Syndesmotic’ injury aka high ankle sprain being a common injury in collision sports, can be a challenging injury to overcome as sometimes it is difficult to diagnose accurately and the mismanagement leads to chronic issues like persistent pain and instability during playing. This injury is no walk in the park compared to other injuries, as the athletes miss about 6 to 8weeks of playing time, which is up to one half of the entire regular session!
WHAT IS HIGH ANKLE INJURY?
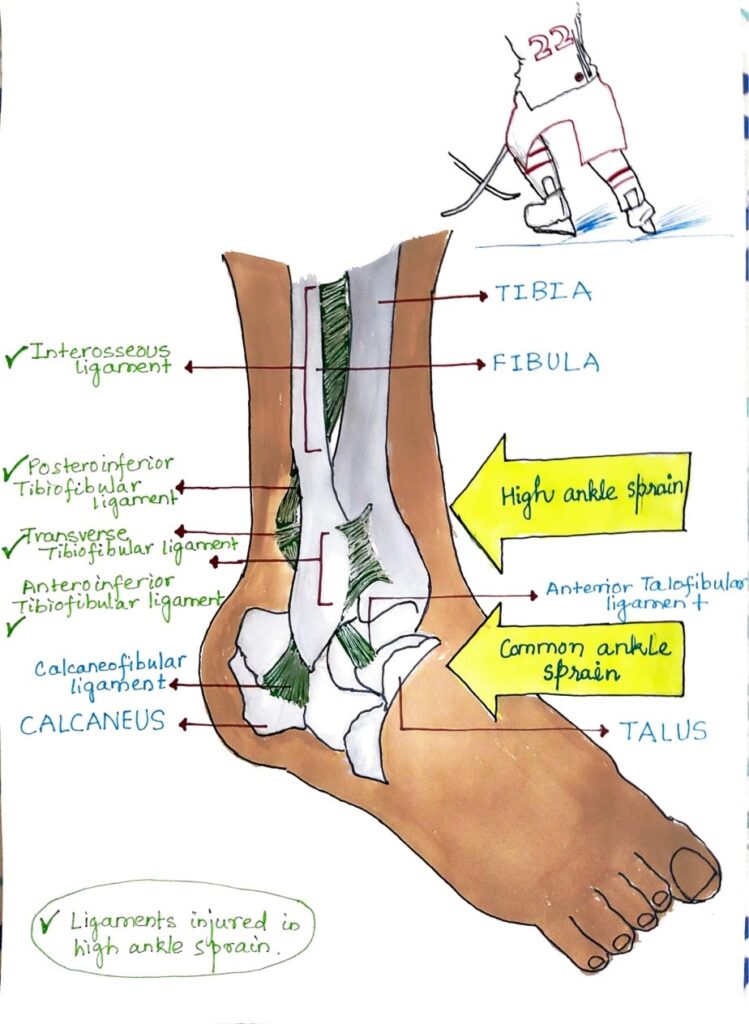
In contrast to lateral ankle sprain, the high ankle sprains occur higher up the foot, above the ankle joint. ‘Syndesmosis’ refers to a fibrous joint between two bones (in this case lower part of tibia and fibula of the leg) that is held together by strong ligaments, with very little to no movement, thus maintaining the stability. So, a high amount of force is needed to injure the ligamentous structures. The ligament surrounds and hence compromised in the injury are the Anteroinferior Tibiofibular ligament (AITFL), Posteroinferior Tibiofibula ligament (PITFL), Transverse Tibiofibular ligament, Interosseous ligament and sometimes the deltoid ligament which is present on the medial side of the ankle joint.
DIFFERENCE BETWEEN HIGH ANKLE SPRAIN AND LATERAL SPRAIN
| TYPE OF ANKLE SPRAIN | LATERAL SPRAIN | HIGH ANKLE SPRAIN |
| Prevalence | Much more common (85%) | Less common (10%) |
| Mechanism of injury | Inversion and plantar flexion | Eversion and dorsiflexion |
| Return to play | Usually faster | Usually slower |
| Structures involved | ATFL, PTFL, calcaneofibular ligament | AITFL, PITFL, interosseous membrane, deltoid ligament |
Timeline for healing based on type of sprain
| Grades of sprain | 0-3d | 4-14d | 3-4wks | 5-7wks | 2-3mo | 3-6mo | 6-12mo | >1yr |
| Grade I | ||||||||
| Grade II | ||||||||
| Grade III | ||||||||
| Intra-articular | Unlikely to heal |
REHABILITATION PROTOCOL
EARLY PHASE
- Immobilize and protect – avoid movement that strains the injured soft tissues like ankle dorsiflexion and foot eversion. For joint protection, initially orthoses like walking boots or ankle stirrup can be used.
- Weight bearing – for grade I, weight bearing can be ensured right away, but for grade II, partial weight bearing with a crutch should be followed for 2 weeks.
- Heel splints – practice to relatively limit ankle dorsiflexion so that once you are able to bear weight, dorsiflexion can be restored in a closed chain for optimal functioning of foot.
EARLY PHASE EXERCISE
- P – Protection
- OL – Optimal loading
- I – Ice
- C – Compression
- E – Elevation
- Ankle pumps
- AROM ankle inversion and eversion
- Toe flexion – extension
- Standing weight shifts
MIDDLE PHASE EXERCISES
- Y balance exercises on foam pad
- Single leg balance – band, anti-eversion
This is a challenging workout for the ankle to resist eversion movement. Graded exposure to movements that has caused the injury is an important part of rehabilitation, especially for players.
Y balances exercise on foam pad



Single leg balance – band, anti-eversion


LATE PHASE EXERCISES
- Return to plyometric movements
- Cutting, running and activity-specific re-integration
- Plyometric progressions – double leg landing mechanics, single leg squat catch, lateral bounding band.
Lateral bounding band


Bounding is a good way to progress the loading on the ankle at the frontal plane, once the sagittal plane movements have become easier.
Single Leg Squat Catch – BOSU


This type of more advanced proprioception drill is needed to be implemented in the later stages of rehabilitation.



{kind=link}